
Assessment in the health and fitness setting can be tricky, and rife with numerous (common) mistakes some fitness professionals make.
This is especially true when we start talking shoulders.
Mistake #1: the shoulder isn’t just the shoulder.
As in: it’s not just one “thing.” We’re actually referring to a shoulder “complex” that’s, well, complex.
The “shoulder” is comprised of four separate articulations (glenohumeral joint, sternoclavicular joint, acromioclavicular joint, as well as the scapulothoracic joint), all playing nicey-nice together in order to perform a wide array of movement(s).
All deserve their time under the assessment microscope.
Mistake #2: However, while all areas are important, I do find that assessing and addressing scapular function/positioning is often the key to unlocking answers.
Unfortunately, it’s often the area that’s least looked at with regards to shoulder pain/dysfunction.
Mistake #3: shoulder assessment can – and should be – attacked from a few different perspectives.
Far too often, I find, fitness professionals take a static view of what’s going on and that’s it. They’ll have an individual stand there in the middle of a room, utter a few “mmm’s and ahhh’s,” write a few fancy schmancy words like “internally rotated,” “kyphotic,” or “I have my work cut out for me,” and that’s that.
Assessment complete.
Lets go squat!
When in fact, shoulder assessment should be broken down into a few disparate – but not altogether separate – components: Static Assessment, Integrative Assessment, and Dynamic Assessment.
Not to mention one’s ability to fill in a smedium t-shirt. Very important.
All three provide pertinent information that will help better ascertain the appropriate plan of attack when it comes to movement dysfunction, pain, and/or improved performance within the shoulder complex.
I Got 99 (Shoulder) Problems and….
…..My scapulae are the reason for all of them.
Sorry, I’m no Jay-Z. And I know I just butchered one of his classic hits.
But it was the only way I could think of to best articulate my point.
The scapulae (shoulder blades) are kind of a big deal when we begin to discuss shoulder health. It’s an arbitrary number I’m throwing out there with no research to back it up – so please, don’t quote me1 – but 90-95% of the “shoulder” issues I’ve helped address in the past when I was a coach at Cressey Sports Performance as well as the present (now that I am on my own), can be correlated back to scapular positioning and function.
Static Assessment
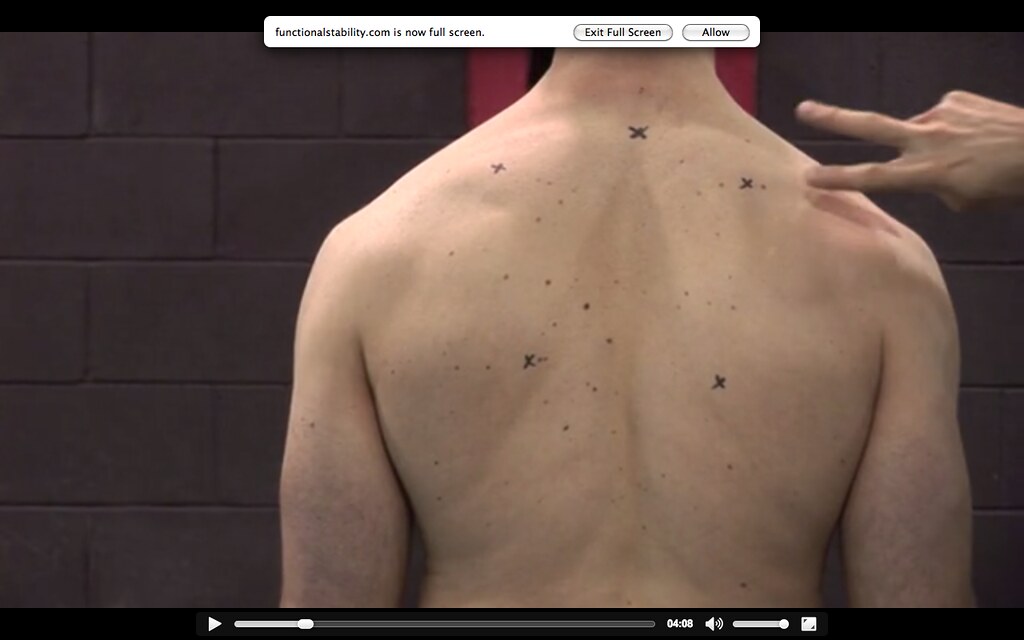
- The scapulae should be in slight upward rotation. As you can see in the picture above, this individual is in slight downward rotation statically (both inferior medial borders (the two bottom x’s) of the scapulae are inside the superior medial borders.
- Both scapulae should rest between T2-T7. The top middle “x” is T2 and you can see this person is below that point and in slight shoulder depression.
- The medial borders themselves should rest between 1-3 inches from the spine.
If we only used static assessment it would be easy to assume this person is f****d. Many fitness pros would see this, hyperventilate into a brown paper bag, and immediately go into corrective mode.
But as Mike Reinold has poignantly noted time and time again:
“Statically, everyone’s shoulder blades start in a different position (elevated vs. depressed, internally rotated vs. externally rotated, abducted vs. adducted, anteriorly titled vs. posteriorly tilted, Autobots vs. Decepticons), and it’s moot to take static posture at face value.”
Besides, the above picture is of me, and when this was filmed/taken I presented with zero shoulder pain. This isn’t to imply I don’t have anything to work on, but it does showcase that static posture alone isn’t going to tell you all you need to know.
Integrative Assessment
Once we start adding movement – looking at scapulohumeral rhythm (the interplay between humerus and shoulder blade) or one’s ability to elevate arms above their head – sometimes, people self-correct really well.
What presents as “bad, “faulty,” or “shitty (<— depending on your rating system) statically, may very well be passable or very good once you add movement.
When looking at shoulder elevation/flexion, for example, does the scapula posteriorly tilt, upwardly rotate sufficiently (generally looking at 55-60 degrees of upward rotation), and does the inferior angle wrap around the thorax to the midline of the body?
This is something that can’t be determined if you’re only looking at static posture.
Dynamic Assessment
This is basically the part of the assessment where I ask the person to do stuff. Rather than boring someone to tears poking and prodding for an hour and making him or her feel like a patient, I prefer to get them moving and have them demonstrate certain exercises.
The push-up tells me a lot. Not only does it give me insight on their ability to move their scapulae (many times they’re “stuck” in adduction), but it also provides details on their lumbo-pelvic-hip control.
Because, something like this makes my corneas want to jump into a pool of acid:
Note: I understand the point of the video above was to purposely showcase a bad push-up. Mission accomplished.
More importantly, if someone comes to me with pain present, having them demonstrate how they perform certain exercises provides unparalleled understanding of what needs to be fixed.
A common theme I see amongst many trainees is allowing their shoulders to roll forward during execution of given exercises.
A Brief Review: when we elevate our arms above our heads the shoulder blades posteriorly tilt (hug the rib cage) and upwardly rotate. Reversing the action calls for scapular anterior tilt and downward rotation.
Many people “feed” into excessive downward rotation/anterior tilt by allowing the shoulders roll forward during common exercises like rows, push-ups, curls, and tricep press downs.
Stop It
I Said, Stop It!
The “fix” here is easy:
Me to Client: “Okay, show me how you’d perform a standing cable row and tricep press down.”
Client: “Um, okay.”
[Then proceeds to emulate technique from the videos above.]
“Yeah, that hurts.”
Me to Client: “Stop doing them that way.”
[Puts client in a better position…shoulders rolled back with posterior tilt.]
Client to Me: “Wow, that feels so much better. You’re so smart and attractive.”
That’s Not All
What’s described above is in no way an exhaustive approach to shoulder assessment, but I hope it at least opened your eyes to the notion that it’s more multi-faceted than many give it credit for.
And on that note, I’d be remiss not to point people in the direction of guys like Eric Cressey, Mike Reinold, and Dr. Evan Osar.
Functional Stability Training – Upper Body is an excellent resource for more insight on shoulder assessment and corrective exercise.
Likewise, Dr. Osar’s Integrative Corrective Exercise Approach is an excellent resource.
And, pimping myself up a little bit, I cover the above and many other shoulder related topics in mine and Dean Somerset’s Complete Hip & Shoulder Workshop coming to the Toronto area in a few weeks (1 week left to take advantage of the Early Bird Special), Seattle, and two stops in Europe in May.
Go HERE for dates and to register.
Did what you just read make your day? Ruin it? Either way, you should share it with your friends and/or comment below.
Source: http://tonygentilcore.com/2016/02/common-mistakes-with-shoulder-assessment/


